Studies consistently show that perimenopause is one of the most under-diagnosed and dismissed conditions in women's health. According to a survey by the Menopause Society, only 20% of OB/GYN residency programs include any menopause-specific training. Women with classic symptoms get told they're stressed, depressed, or "just getting older." This guide is about changing that — by walking into your appointment with the data and language that make dismissal much harder.
This article is for informational purposes only and is not medical advice. Always consult a qualified healthcare provider about your symptoms.
Why so many doctors miss perimenopause
Several structural factors explain the dismissal pattern:
- Limited training. Most physicians received minimal menopause-specific education in medical school or residency.
- Time pressure. 10-15 minute appointments don't allow for thorough symptom history.
- Single-test thinking. Doctors look for one definitive test. Perimenopause has no single test — hormones fluctuate too much for a single blood draw to be conclusive.
- Age assumptions. Women under 45 are often told they're "too young" despite 5-10% of women starting perimenopause in their late 30s.
- Symptom overlap. Perimenopause symptoms overlap with stress, thyroid issues, depression, and many other conditions, leading to misdiagnosis.
The good news: you can compensate for all of these by how you prepare for and approach the appointment.
Step 1: Track for 2-3 months before your appointment
The single most powerful thing you can do is bring data. A woman saying "I sometimes feel tired and moody" is easy to dismiss. A woman showing 12 weeks of tracked data showing fatigue clustering in the late luteal phase, hot flash frequency increasing month over month, and sleep quality scoring 4/10 on average — that's much harder to dismiss.
Track at minimum:
- Menstrual cycle (start date, length, flow)
- Your top 3-5 worst symptoms (intensity 0-10 daily)
- Sleep quality and any night sweats
- Mood and energy
- Any new symptoms that have appeared
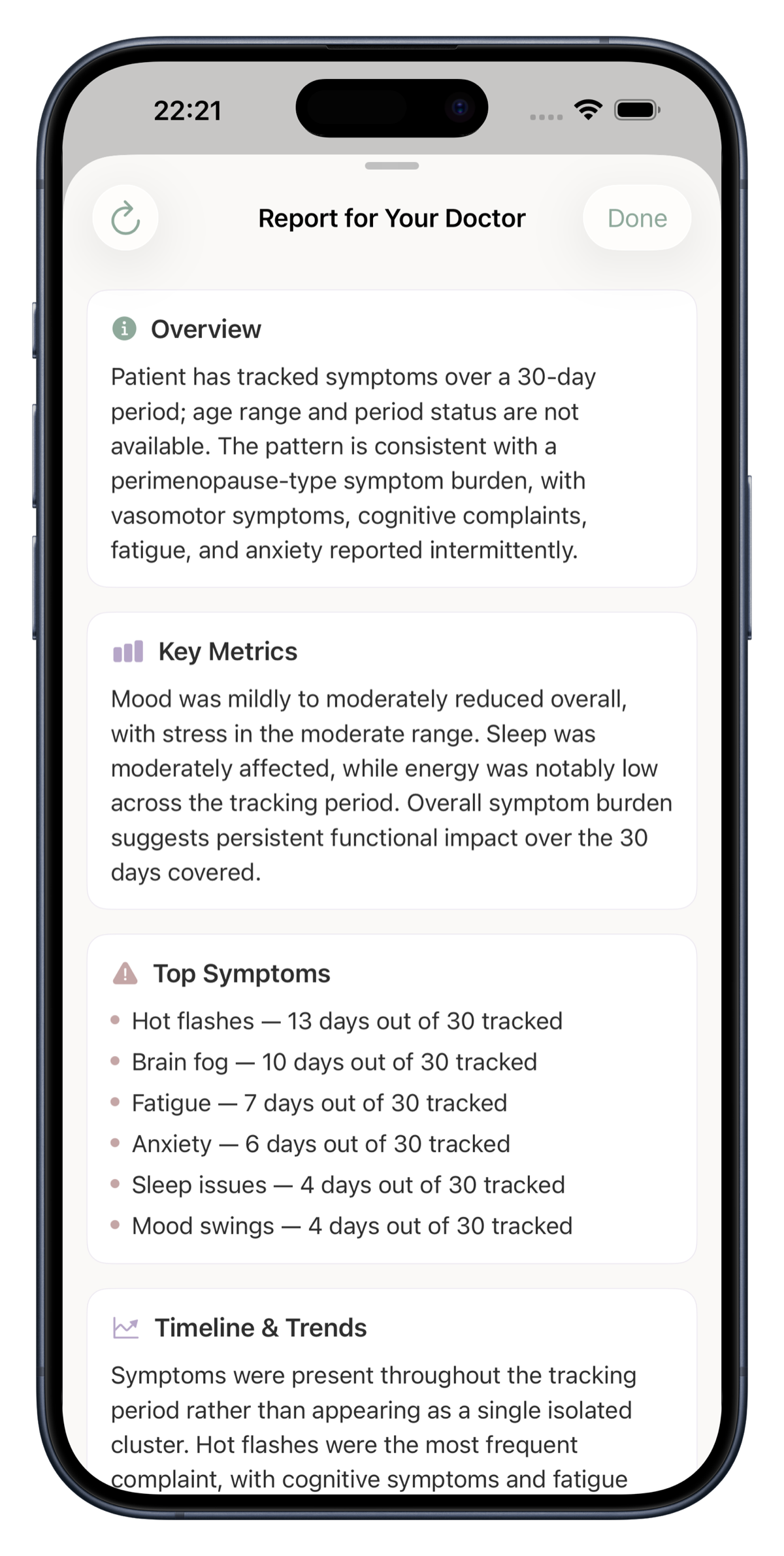
Apps like Perimosa are designed for exactly this — daily 30-second check-ins that generate a doctor-ready report showing your patterns clearly. Without tracking, the patterns are invisible. With tracking, they become the foundation for taking action.
Step 2: Write down your top 3 concerns before walking in
Don't try to remember everything in the moment. Doctors get the most information when patients prepare a focused list. Limit yourself to your top 3 most disruptive issues. This focuses the conversation and ensures the most important things get addressed even if time runs short.
Example list:
- I'm waking at 3am most nights and can't fall back asleep. This has been worsening for 6 months.
- I'm having 8-12 hot flashes daily, including drenching night sweats that ruin my sleep.
- I'm experiencing significant anxiety I've never had before, including occasional panic attacks.
This is much more useful than a 10-minute monologue about everything that feels off.
Step 3: Use clear medical language
The language you use shapes how the doctor responds. Vague descriptions invite vague responses. Medical-adjacent language signals you've done your homework and are taking the conversation seriously.
Less effective: "I'm feeling off, like something's wrong, I don't know what's happening to me."
More effective: "I believe I may be in perimenopause. I've been experiencing classic symptoms including vasomotor symptoms (hot flashes and night sweats), sleep fragmentation with characteristic 3am wakings, new-onset anxiety, and cycle changes — my cycles have varied from 24 to 35 days over the past 4 months. I'd like to discuss evaluation and treatment options."
This framing shifts you from being a patient with vague complaints to a patient presenting a clear clinical picture.
Step 4: Request specific blood work
Many doctors will order TSH and call it a day. Request a more thorough panel:
- FSH on cycle day 2-3, repeated 6-8 weeks later (single test can miss perimenopause because levels fluctuate dramatically)
- AMH — anti-Müllerian hormone, a more stable marker of ovarian reserve
- Estradiol on the same days as FSH
- Full thyroid panel: TSH, free T3, free T4, and TPO antibodies (thyroid issues frequently co-occur and get missed when only TSH is checked)
- Prolactin
- Fasting glucose and A1c — insulin resistance affects perimenopausal women significantly
- Ferritin — not just hemoglobin (iron stores often run low long before anemia shows, especially with heavy perimenopausal bleeding)
- Vitamin D 25-OH — deficiency mimics and worsens perimenopause symptoms
- Vitamin B12 — absorption decreases with age, deficiency causes fatigue and brain fog
According to The Menopause Society, this kind of comprehensive workup is standard for symptomatic perimenopausal women. If your doctor refuses parts of this, ask why specifically and request a referral.
Step 5: Ask the right questions
Questions to ask:
- "Based on my symptoms and history, do you think this could be perimenopause?"
- "What testing would help clarify whether I'm in the menopausal transition?"
- "What are my treatment options for [your specific worst symptoms]?"
- "Is HRT appropriate for me? What are the risks and benefits given my personal history?"
- "What non-hormonal options exist if I prefer those or can't use HRT?"
- "When should I follow up with you to assess whether treatment is working?"
What to do if your doctor dismisses you
Common dismissal patterns and how to respond:
"You're too young for perimenopause." Respond: "About 5-10% of women begin perimenopause before 40. I'd like to be evaluated for it specifically rather than ruled out based on age."
"It's probably stress/anxiety. Try managing stress better." Respond: "I understand stress can contribute. I'd also like to rule out hormonal and other medical causes. Could we run a thorough workup to be sure?"
"Your blood tests look normal." Respond: "I understand a single test can miss perimenopause because hormones fluctuate. Could we repeat the FSH in 6-8 weeks, and also check the broader panel including AMH and the metabolic markers?"
"You're just going through normal changes. Wait it out." Respond: "These symptoms are significantly impacting my quality of life. I'd like to discuss treatment options rather than wait. The 'window of opportunity' for HRT is now and I want to make an informed decision."
If after a respectful but persistent conversation your doctor still won't take you seriously, request a referral to a gynecologist or menopause-trained specialist. The Menopause Society directory lists certified practitioners by location.
Finding a menopause-trained doctor
Menopause-trained doctors take a different approach than general primary care for these symptoms. They're familiar with current treatment options, the nuances of HRT initiation timing, and the wide range of non-hormonal options. They typically don't dismiss based on age.
Options:
- The Menopause Society directory — searchable by location
- Telehealth menopause services (Midi Health, Alloy Health, Evernow, Gennev) — useful if local options are limited
- OB/GYNs who advertise menopause specialization
- Referrals from women in your network who've had good experiences
The Bottom Line
Getting taken seriously by a doctor about perimenopause requires preparation. Track your symptoms systematically for 2-3 months. Write down your top 3 concerns. Use clear medical language signaling you've done your research. Request comprehensive blood work, not just TSH. Ask the right questions. And if you still get dismissed, find a menopause-trained specialist. The current generation of women refuses to accept dismissal — that's how the standard of care shifts. Your data and your voice are part of that shift.